On 9 January 2021, a Boeing 737-500 aircraft, registration PK-CLC, was on a scheduled domestic flight, from Soekarno-Hatta International Airport (WIII), Jakarta, to Supadio International Airport (WIOO), Pontianak. PT Sriwijaya Air flight SJ182 crashed into the sea about five minutes later, with all 62 lives lost in the tragedy. Weather conditions for the mid-afternoon flight were not considered a factor.
The Captain was the pilot flying (PF). The 54 year old Captain had nearly 18,000 flight hours, over 9,000 in the 737. The 34 year old First Officer, pilot managing (PM), had over 5,000 flight hours, virtually all on the 737.
KNKT, Komite Nasional Keselamatan Transportasi is the Indonesia Independent Investigation Authority also known as National Transportation Safety Committee / NTSC) released the final accident report on 10 Nov 2022.

PK-CLC, a 737-500 delivered in 1994 to Continental Airlines, was included in a complex mandate to enhance flight data recording. The FAA considered the 737 a special case because of its multi-generational longevity and because of the sheer numbers.

PK-CLC was upgraded with ADS-B while being stored. It returned to service on Dec. 19. The airplane was a workhorse, with about six flights a day, every day. Jan 9 was the 22nd day into service, with over 130 flights completed.
The figure below is annotated from the flight data published in the final report.
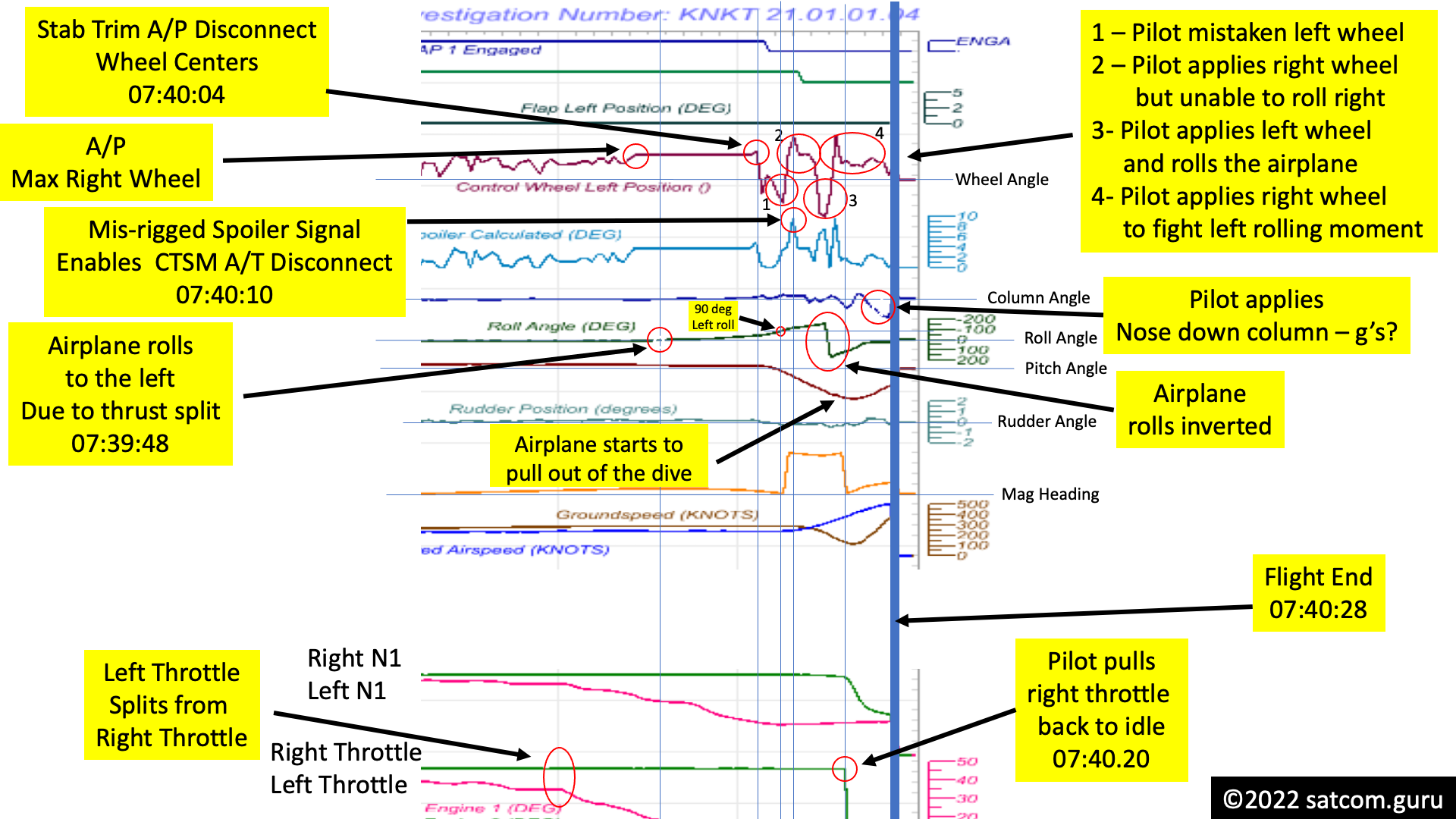
The 737 autothrottle malfunctioned when the right throttle "stuck" at climb power while the left throttle was reduced, causing a thrust asymmetry and resultant left yawing moment. The yawing moment translated into a left rolling moment. The autopilot was commanded to turn the airplane to the right and applied increasing right wheel (right rolling moment via aileron command) to cause the airplane to bank to the right. The thrust asymmetry left rolling moment overwhelmed the autopilot right aileron command and the airplane began to bank to the left, in spite of the significant right wheel command.
As the bank angle to the left increased, and as the thrust asymmetry increased, a "BANK ANGLE" aural alert was generated. The Captain momentarily triggered the stab trim which caused the autopilot to disconnect and to cause the wheel to return to center. The Captain, perhaps confused by the persistent significant right wheel command and thought the airplane was excessively banked to the right, applied left wheel command, which further banked the airplane to the left to about 90 degrees.
At this point, the Captain, perhaps finally taking note of the actual airplane attitude, applied significant right wheel command to try and recover to wings level. However, as the airplane was now descending and accelerating, the autothrottle was further reducing the left throttle and increasing the opposing thrust asymmetry left rolling moment in opposition. The result was the airplane did not roll to the right and remained at extreme left bank.
The Captain, now faced with no option, applied left wheel and caused the airplane to roll inverted and proceed towards wings level from "the other side". All the while with the throttles split nearly full travel.
As the airplane got back to wings level, the pilot continued to apply right wheel to offset the thrust asymmetry left rolling moment. As the airplane was now diving steeply, someone (the Captain) reduced the right throttle to idle, and the thrust asymmetry began to reduce, allowing the pilot to relax the opposing right wheel.
As the airplane approached wings-level, it began to pull out of the steep dive. Pitch angle peaked at -70 degrees. Vertical speed peaked at about -45,000 fpm. Airspeed peaked at around 500 knots.
It took about 23 seconds from the beginning of the dive until crashing into the sea.

In the pullout, vertical speed decreased from -45,000 fpm to about -38,000 fpm in about 3 seconds. That would equate to about a 2.2g pullout. At 2.2g pullout, it would have taken about 13,400 feet of altitude to level out (and they only had 2,000 feet).
The Captain applied nose down column command in the pull-out which is entirely the opposite of what would have been expected. Normally pilots pull back with all their strength in such a scenario. The Captain needed to pull-out much more aggressively to have any chance of survival.
It would have taken at least a 5.4g pullout to level out in the remaining 2000 feet of altitude from -45,000 fpm. Whether the airplane could have taken the loads, and at such extreme overspeed, is uncertain, but not inconceivable. In any case, the pilot had no time to waste.
737 throttle split has been a continuing issue with 737.
From the KNKT accident report:
The Cruise Thrust Split Monitor (CTSM) disengages the A/T when A/P roll control requires significant spoiler deployment and a disparity of calculated thrust (in A/T computer) of both engines when at the same time, normally the thrust levers become separated. The CTSM is active when flaps are less than 12.5°, and the A/T is not engaged in the takeoff or go-around mode.
On 16 November 2000, the FAA issued Airworthiness Directive (AD) number FAA AD 2000-23-34 to replace the existing A/T computer with a new P/N. The FAA AD refers to the Boeing Service Bulletin number SB 737-22A1130 dated 24 September 1998.
The AD was applicable to all Boeing Model 737-300, -400, and -500 series airplanes was effective from 8 January 2001. The AD referred to Boeing Alert Service Bulletin number 737-22A1130 which required replacement of the previous A/T computer with improved A/T computer Boeing P/N 10-62017-30 or 10-62017-31.
The AD addressed the problem of split thrust lever movement caused by irregular A/T operation which results in asymmetric thrust conditions causing the airplane to bank excessively and going into a roll.
CTSM was installed on this airplane. CTSM should have caused the autothrottle to disconnect.
The FDR recorded at 07:39:40 UTC, the control wheels deflected to the right about 19°, the left aileron deflection down 3.3° and the right aileron deflected up 5.8°, the calculated spoiler deflection was 3.7°, and the aircraft roll angle was 15° to the right. Based on the CTSM design, the A/T should have been disengaged at this time as all requirements were met.
The autothrottle did not disconnect at 07:39:40, but much later at 07:40:10. Had the autothrottle disconnected as designed, the autopilot would have still had remaining right rolling moment authority and control would not have been lost.
The investigation concluded that the spoiler position sensor that was used in the CTSM monitor was mis-rigged. At the point that the autothrottle disconnected, which was presumably by CTSM command, the spoiler sensor position was much higher than what should have been needed to trip the monitor.
The FDR did not record A/T manual disconnection at the time of the A/T disengaged, meaning that the disengage button on either thrust lever was not used by the crew to disengage the system. While it is possible for the A/T to be manually disengaged using a switch on the MCP, this would not be an expected technique during an upset recovery event. In addition, during the accident flight the thrust levers were not manually moved until 9 seconds after the A/T disengaged. It would seem unlikely that the crew would disengage the A/T manually but then waited 9 seconds to move the thrust levers.
There were seven recorded thrust asymmetry events uncovered by reviewing flight data from 2013 onwards. One of these events recorded the same autothrottle disconnect condition.
The QAR data of the flight on 15 March 2020, revealed the same A/T disengagement signature as the accident flight. On this flight the control wheel deflection recorded on the FDR around the time of the first A/T disengagement was between 15° and 36° to the right, which corresponds to a calculated spoiler deflection of between 2.15° and 10.88°. The control wheel deflection recorded around the time of the second A/T disengagement was between 32° and 28° to the right, which corresponds to a calculated spoiler deflection was between 9.22° and 7.38°. In both the 15 March 2020 event and the accident event the disconnect occurred at the time when the control wheel first moved beyond the autopilot saturation position.. The QAR also did not record A/T manual disconnection and it would be even less likely that the MCP disconnect switch would be used in both upset events.
In both the 15 March 2020 event and the accident event the A/T disengaged timing showed that, the disengagement occurred at the time when the control wheel moved beyond the A/P saturation position of 5.75° deflection.
The spoiler position sensor was never checked by the airline, as no declared circumstance had occurred requiring it.
The investigation could not determine the cause of the flight spoiler signal value being too low. The multiple sources that possibly caused a too low of the flight spoiler signal value, including a mis-rigged or erroneous spoiler sensor, mis-rigged spoiler actuator, or a sheared or damaged spoiler linkage.
The Sriwijaya Air advised to the investigation that flight spoiler sensor rigging had never been performed on PK-CLC aircraft while being operated by Sriwijaya Air as it never met the requirement to do so.
In-spite of the seven occurrences of throttle split, none were ever reported. Furthermore, somewhat incredulously, pilots failed to observe the physical throttle splits, instead picking up the thrust asymmetry via engine indications.
The QAR data showed 7 occurrences of thrust levers split prior to the accident and based on the interviews none of the pilots noticed these until other indications were detected. The simulations performed in Jakarta and Las Vegas showed that the pilots did not realize the thrust levers split, until they noticed the engine parameters when they scanned the instrument panels. The thrust levers positions that were split might not have been monitored by the pilots as no engine power change required during this phase of the flight.
One of the seven occurrences, on 15 March 2020, in an tragic irony, involved the Captain of the accident flight (he was pilot monitoring on that flight).
The PIC of this flight was the PF of the accident flight. The investigation conducted an interview with the SIC of this flight.
The SIC recalled that during the flight, he acted as PF and while maintaining altitude of 5,000 feet, the ATC provided clearance to turn to the right. The SIC turned the heading selector on the MCP and noticed that the aircraft was unable to turn to the right. The SIC reported the condition to the PIC. The SIC then disengaged the A/P and turned the aircraft manually. After few moments the PIC realized that asymmetric thrust occurred, and the left thrust lever was at the idle position. Thereafter, both thrust levers restored to about 25° position, the aircraft returned to normal condition and no further anomalies occurred until landing. The SIC did not recall any additional details of the flight. Investigators were unable to determine how the PIC diagnosed the asymmetric thrust condition.
No pilot report of aircraft system malfunction was filed into the AML nor safety occurrence report to the operator safety reporting system.
In five of the seven cases, the right throttle became unstuck without pilot intervention. In all five of these cases, neither pilot was aware of the circumstance and made no report, of course.
Pilots did take notice and action in two of the seven flights: 15 March 2020 (above) and 7 January 2021 (below).
The investigation team has interviewed both pilots of the flight. Both pilots stated that they noticed fuel unbalance and thereafter noticed thrust lever asymmetry. The pilots disengaged the A/T, adjusted the thrust levers manually to about equal position and re- engaged the A/T. The A/P remained engaged during the asymmetric event occurred.
No pilot report was filed into the AML after this flight.
A point of Flight Operation Quality Assurance (FOQA) is to detect unsafe conditions that might not have been reported. There were many opportunities for the mis-rigged spoiler to be detected if only someone had been looking for it (thrust split without autothrottle disconnect). That the Captain had the opportunity to save himself about ten months later is profoundly discouraging.
Service history for the autothrottle was tabulated from 2012 to the accident.
The 65 pilot reports related to the A/T system mainly consisted of the following:
- A/T system cannot be engaged
- A/T system disengage during flight
- A/T system could not hold in ARM position
- A/T unserviceable.
48% of the corrective action taken was cleaning contacts.
...cleaning of the electrical connector of the A/T system components followed by performing the Built in Test Equipment (BITE) procedure to clear faults.
The AML record showed that some of the reported problems appeared to be solved after the electrical connector cleaning was performed. The record also showed that after the engineer cleaned the electrical connector, the BITE tests were performed which showed the result of “no faults” and the rectification actions were stopped.
Digital computer systems are very capable to detect failures and report them. However, powering a unit up on the ground and running the power-up tests does not necessarily encounter the circumstances that may create a failure. The issue is to exercise the autothrottle in a manner that can detect all these failures, and that can become time-consuming and conflicting.
The saying, "problems that go away by themselves, come back by themselves", should be entrenched in safety management. Yet, the pressure to return to service, along with culture and in-experience, finds this compromised. It is rolling dice with tragedy on the line.
The termination of the trouble shooting after the BITE test result of “no faults” and without the pilot report of thrust lever split, resulted in the engineers stopped the trouble shooting steps and not proceed to examine the engine thrust control as required in AMM chapter 71-00-49. This is likely the reason why the defect prolonged.
In summary:
- Throttle split due to binding is a recurring problem on 737
- CTSM was installed to prevent the autothrottle from creating excessive throttle split
- CTSM spoiler input appears to have been mis-rigged. There was no reported event that required checking the alignment.
- FOQA data had evidence of throttle split and CTSM malfunction, but there was no awareness
- At least two flight crews previously noted throttle split, but made no report that could have uncovered the spoiler mis-rigging.
- During the accident flight, the PF and PM did not make take any action or had any apparent awareness of the throttle split until far too late to recover
- During the accident flight, the PF and PM did not take any action or had any apparent misgiving from the persistent autopilot command of right wheel, or the inability to turn right as commanded.
- During the accident flight, the PF took the opposite action responding to the BANK ANGLE alert, much worsening the bank angle exceedance.
- During the accident flight, the PF fought the thrust asymmetry when unsuccessfully trying to roll right to airplane wings-level without any action to reduce the thrust asymmetry. This further delayed recovery and much worsened the dive.
- During the accident flight, the PF elected to completely roll the airplane through inverted to recover rolling left without any action to reduce the thrust asymmetry until nearing wings-level. This much worsened the dive.
- During the accident flight, the airplane pull-out was about 2.2g but hit the sea still going about -38,000 fpm.
On 25 March 2022, Boeing published a revision to the Maintenance Planning Document (MPD) for the 737-300/-400/-500 requiring repetitive inspections on the spoiler and aileron deployment and associated position sensors. Boeing is developing a service bulletin to address a pending Airworthiness Directive mandate of an initial inspection to be performed within 250 flight hours of the issuance of the service bulletin and repetitive tests of the spoiler deployment and aileron position sensing not exceeding a 2,000 flight hours interval.
The airline took a number of safety actions, one to add a monitor for thrust asymmetry.
Revised the Flight Data Analysis (FDA) event to include thrust asymmetry and Loss of Control in flight events
Performed thorough A/T and spoiler inspection on Boeing 737-500 registered PK-CLE to ensure the correct function of the system. The inspection also planned for Boeing 737-800 fleet.
Other actions taken included pilot training (upset recovery) and maintenance monitoring, procedures and training.
There was a strange issue with the Cockpit Voice Recorder, still unresolved.
The Cockpit Voice Recorder (CVR) equipped in the aircraft only recorded the PIC voice when the voice was loud enough to be received in the in the SIC’s headset microphone, and the channel of cockpit area microphone only recorded a prominent tone with a frequency of around 400 Hz which interfered all other audio.
The CVR downloaded in 2019 for renewal of the C of A, found the Channel 4 recorded a tone with a frequency of 400 Hz. The CVR download in 2020 found that the Channel 4 recorded conversation between engineers. The result for both downloads stated that the CVR was functioning correctly. The investigation was unable to determine the reason of why Channel 4 recorded a prominent tone with a frequency of about 400 Hz in 2019 and the accident flight while the recording that were downloaded in 2020 were normal.
The flight crew failed to detect the throttle split. The Captain initially took the wrong action responding the BANK ANGLE alert.
The investigation concluded that during the accident flight, the pilots should have enough time to monitor the thrust lever asymmetry and able to recognize deviation of the flight path. However, the pilots did not identify the flight anomaly before it developed into an upset condition. This lapse of not identifying the anomaly could be due to reduced active monitoring because of pilot automation complacency and confirmation bias that aircraft was performing the right turn as commanded. Without using the EADI as primary reference in assessing the aircraft attitude, the pilot was not able to apply correct recovery inputs.
I published a report from my analysis of SJ182 Flightradar24.com ADS-B data on the day after the accident.
https://www.satcom.guru/2021/01/sriwijaya-air-flight-sj182.html
Please take note of how accurate the ADS-B analysis matched the fight recorder data. I was able to detect that the airplane had suffered a lateral upset, and had rolled inverted in the upset based, based on the very limited data set. My conclusions from that moment:
- the airplane appears to be operated normally up to the event
- a lateral upset causing the airplane to turn in the opposite direction appears to be the trigger
- the airplane nosed over and proceeded into a steep dive, with airspeed increasing well above normally operating limits.
- while in the dive, the airplane began to turn to the right.
- One explanation for this behavior is that the airplane initially rolled to the left, inverted, and continued towards wings level, impacting while still turning right.
No comments:
Post a Comment